
Eric Karas, Neal Masia
As many as 2 in 3 children and 1 in 4 adults experience needle phobia, introducing significant challenges for treating anaphylaxis. Anaphylaxis is a severe and potentially life-threatening allergic reaction that can occur in response to certain allergens, such as foods, insect stings, medications, or latex. It often involves symptoms like difficulty breathing, swelling of the face and throat, and/or a drop in blood pressure, and it can progress rapidly. Immediate medical attention is crucial in cases of anaphylaxis, typically involving the use of epinephrine and other supportive treatments. Until last year, only injectable epinephrine was available for this type of emergency use, but fear and discomfort with needles has been problematic in its administration. In addition to formal patient preferences research, analysis of videos and posts on social media platforms show widespread fear of receiving and using epinephrine auto-injectors (Kafal et al., 2024; Martel et al., 2023).
EntityRisk has been working with ARS Pharma over the past three years to demonstrate the societal value of their product neffy®, which as of August 2024 was the first nasal spray for treating anaphylaxis with epinephrine. With the impending launch of neffy®, ARS was confident in the clinical and practical differentiators of neffy® from branded and generic epinephrine auto-injectors, particularly the advantage of needleless administration, but it was unclear to what degree they impacted the value of the product, and therefore, neffy®’s value-based price (VBP).
EntityRisk and ARS conducted an economic analysis to estimate the range of supportable prices for neffy® commensurate with its societal value using generalized cost-effectiveness analysis (GCEA) methods to best reflect the value for real patients, particularly in the case of severe conditions like the risk of anaphylaxis. We took an approach to incrementally measure potential sources of value to the VBP calculation to understand the impact of each independently and together.
Model and methods:
To estimate the value of neffy®, we constructed a cohort model aligned with the (at the time) proposed model for ICER’s Peanut Allergy Study (Tice et al., 2019). The model follows the lifetime health and spending outcomes (up to 90 years) of a cohort of patients at risk for anaphylaxis and using neffy®, compared to the corresponding outcomes of at-risk patients using branded EpiPen auto-injector devices. Health impacts are summarized in terms of quality-adjusted life-years (QALYs), which represent life-years scaled by an estimate of health-related quality of life (Institute of Clinical and Economic Review, 2020).
We modeled the effectiveness of both neffy® and EpiPens as improving health by treating anaphylaxis. Clinical effectiveness was assumed to be the same for EpiPen and neffy® when used within the “golden window,” typically thought to be 5 minutes from the onset of anaphylaxis (Armstrong et al., 2013). However, key differences across carry rates, proper use, shelf-life, and quality of life (QoL) were considered. To compute QALYs, estimates of health-related quality of life (HRQoL) were needed for each relevant health state. Baseline HRQoL and several HRQoL scenarios were explored
to evaluate the HRQoL decrement of needle aversion captured in carrying a needle daily and using a needle in the event of a severe reaction. Direct medical costs included primary care provider and food allergy specialist visits twice per year (Cannon, 2018). Severe reactions included costs for emergency department admission, hospitalization, and ambulance transport1. GCEA also facilities the inclusion of non-medical costs due to diet changes (Cannon, 2018) and productivity2 (Cannon, 2018; Bureau of Labor Statistics). Finally, cost of treatment with neffy® was compared to the EpiPen net price of $300.
1 Severe reaction medical costs were computed from 2019 Medical Expenditure Panel Survey (MEPS) data. Per patient hospitalization costs, emergency room visit costs, primary care provider visits, other outpatient visits, and ambulance costs associated with an ICD-10 code of T78 are estimated.
2 Productivity costs are estimated as the days of work lost due to anaphylaxis events (Cannon, 2018) multiplied by the US average daily wage (Bureau of Labor Statistics).
Findings:
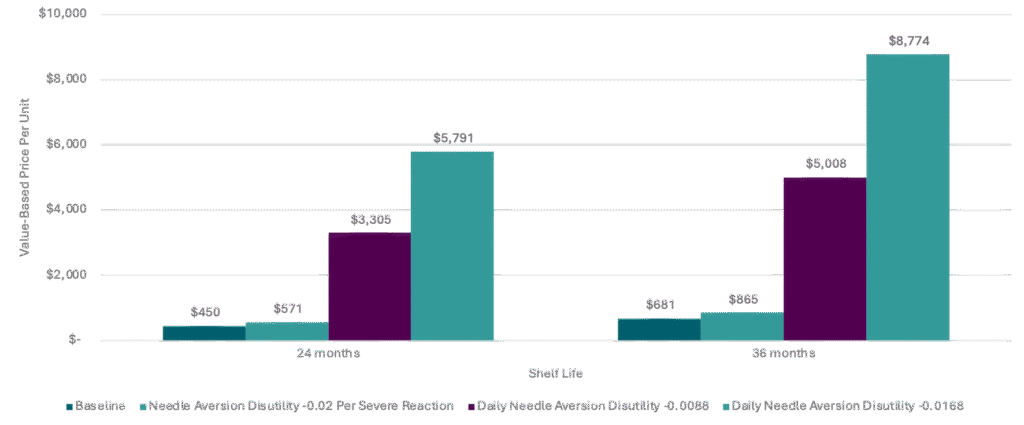
While we explored many additional value drivers, we found the VBP to be most impacted by shelf-life and quality of life improvements due to needleless administration; therefore, these results are focused on the incremental value generated from neffy®’s shelf-life and various needle aversion estimates.
Relative to EpiPen, economically supportable prices for neffy® ranged from $450 with the baseline quality of life and a 24-month shelf-life to over $8,000 when accounting for maximum needle aversion disutility and a 36-month shelf-life.
Disutility per severe reaction increased the VBP by over 25% from baseline, but incrementally adding daily disutility had a more substantial increase on the VBP—over 6x to nearly 13x from baseline.
Conclusions:
The principal source of economic value from neffy® is the benefit offered to patients with aversion to needles, which was initially hypothesized based on the existing literature and later substantiated with a patient preference study to estimate the magnitude of the benefit.
Importantly, GCEA allowed for inclusion of key value differentiators that are therapeutic area, product, and patient population-specific. Other factors, such as carry rates, adherence rates, and timely use were explored, but they had limited impact on VBP compared to shelf-life and needle aversion. The effect of dynamic pricing, accounting for price drops due to loss of patent exclusivity over the course of neffy®’s lifetime, though not included in these results, would also increase the VBP.
While economically supportable prices for neffy® range from $450 to over $8,000, it is of utmost importance to ARS that neffy® be accessible to patients in need of carrying a treatment for anaphylaxis daily, aligning with preferences around needleless epinephrine administration.
References
Armstrong, N., Wolff, R., van Mastrigt, G., Martinez, N., Hernández, A. V., Misso, K., & Kleijnen, J. (2013). A systematic review and cost-effectiveness analysis of specialist services and adrenaline auto-injectors in anaphylaxis. Health Technology Assessment (Winchester, England), 17(17), 1–117.
Cannon, H. E. (2018). The economic impact of peanut allergies. Am J Manag Care, 24(19 Suppl), S428-33.
Institute for Clinical Economic Review. (2020). 2020-2023 value assessment framework. Institute for Clinical and Economic Review Cambridge. https://icer.org/wp-content/uploads/2020/10/ICER_2020_2023_VAF_102220.pdf
Kafal, Ayman, Autumn Burnette, Nicole Chase, Daniel Soteres, Bob Geng, Harris Kaplan, and Sabera Hyderally. 2024. A Survey of Allergists, Pediatricians, and Primary Care Physicians About the Utilization of Epinephrine, Journal of Allergy and Clinical Immunology, 153: AB76.
Martel, T, L Mitchell, and D Gardner. 2023. Exploring the Interplay of Epinephrine and Needle Phobia: Implications and Strategies, Annals of Allergy, Asthma & Immunology, 131: S74.
Tice, J. A., Herron-Smith, S., Tsiaso, E., Chapman, R., Zaim, R., Segel, C., Rind, D., Pearson, S. D., Guzauskas, G. F., & Hansen, R. N. (2019). Oral Immunotherapy and Viaskin® Peanut for peanut allergy: Effectiveness and value. Institute for Clinical and Economic Review. https://icer.org/wp-content/uploads/2020/10/ICER_PeanutAllergy_Final_Report_071019.pdf
United States Bureau of Labor. (2023). The Employment Situation—June 2023. https://www.bls.gov/news.release/empsit.t19.htm.


